|
UNIVERSITA'
DEGLI STUDI DI CAGLIARI
FACOLTA'
DI MEDICINA E CHIRURGIA
ISTITUTO DI DISCIPLINE ODONTOSTOMATOLOGICHE
E CHIRURGIA MAXILLO-FACCIALE
SCUOLA DI SPECIALIZZAZIONE IN ODONTOIATRIA E PROTESI DENTALE
Director: Prof. Ignazio MARIA CORTIS
|
|
|
|
|
G.PETTI *, I.M.Cortis,
C.Cortis
*G.PETTI, Professor of Periodontology, Università di Sassari
|
|
|
Published in May-September 1992
|
|
|
|
|
SURGICAL TREATMENT
OF 1st, 2nd AND 3rd CLASS LESIONS OF BI- AND TRIFURCATIONS
|
|
GUSTAVO
PETTI
Physician and Surgeon specializing in Dentistry. Periodontist.
Piazza Repubblica 4, 09129 Cagliari, Italy.
tel ++39 070 498159, fax ++39 070 400164
web site www.gustavopetti.it
|
|
|
|
|
Treatment
of initial 1st and 2nd class lesions of bi- and trifurcations.
|
|
 |
|
|
|
|
|
|
|
|
|
|
 |
|
|
|
|
|
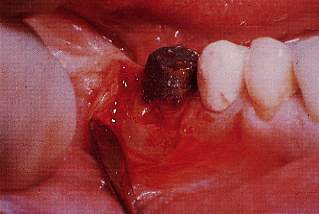
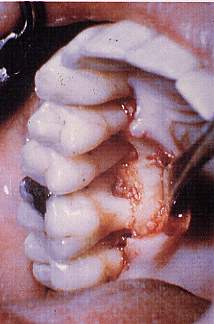
Fig. 1. Severely
damaged bifurcation of 4.6. The probe penetrates 3 mm at the bifurcation. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
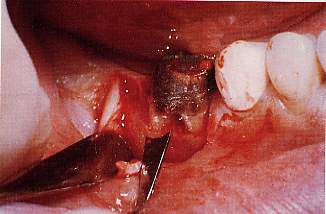
Fig. 2. Osteotomy-osteoplastics
with rotating instruments for use at a distance from roots. |
|
|
|
 |
|
|
|
|
|
|
|
 |
|
|
|
|
|
|
|
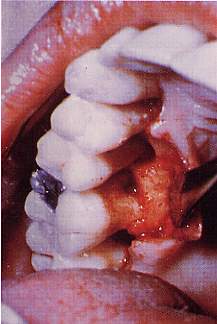
Fig. 3. Osteotomy-osteoplastics
with hand instruments, scalpels, close to roots to recreate festooning. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
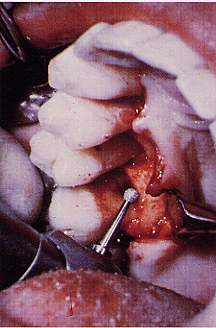
Fig. 4. Osteotomy-osteoplastics
with a file to reconstruct the interradicular furrow as if we were on an
interdental platform between two different roots. |
|
|
|
|
|
|
|
|
 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fig. 6. 1st class
lesion at the trifurcation of 1.6 - the bifurcation between the palatal
root and the mesial vestibular root is involved. There is also a bone defect
at the level of the palatal surface of the root of 1.5, it too curable through
resective bone surgery. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
 |
|
|
|
|
|
|
|
|
|
|
Fig. 5. Bone remodelling
completed: the festoon near the roots has been reconstructed. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fig. 8. The bone architecture
has been restored. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fig. 7. Osteotomy-osteoplastics
with rotating instruments, as if two roots of two different and adjoining
teeth were involved |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Treatment
of advanced 2nd class lesions and of passing 3rd class lesions of bi- and
trifurcations.
|
|
|
|
|
|
|
|
|
 |
|
|
|
|
|
|
 |
|
|
|
|
|
|
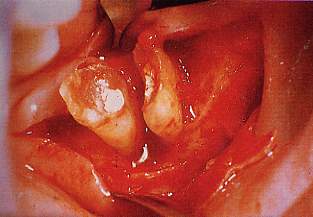
Fig. 9. Serious
coronal damage to 4.7 and passing 3rd class damage to the bifurcation. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
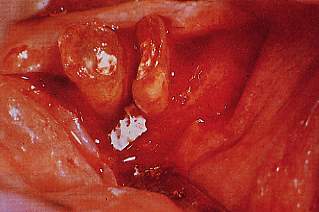
Fig. 10. After sculpting
a mucoperiosteal flap, the roots are separated and a serious interradicular
bone defect appears. |
|
|
|
|
|
|
 |
|
|
|
|
|
 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fig. 12. The
graft with heterologous Kiel bone, once completed, is shaped and the flap
is sutured.odella e si sutura il lembo.
|
|
|
|
|
|
|
|
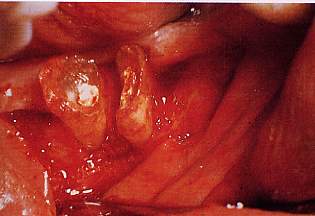
Fig. 11. One proceeds with
osteotomy-osteoplastics and an interradicular bone graft to eliminate the
defect (Petti, 1987). |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
 |
 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|